Muhammad Imran Hussain
Department of Conservative Dentistry, Sir Salimullah Medical College Dental Unit, Dhaka, Bangladesh.
A K M Bashar
Department of Conservative Dentistry and Endodontics, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh.
A H M Zakir Hossain Shikder
Department of Pedodontics, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh.
Keywords: MTA pulpotomy, Acute irreversible pulpitis, HIV-positive patient, Root canal treatment
DOI: 10.3329/bmrcb.v47i2.57785
Abstract
Background: Root canal treatment is the usual management of acute irreversible pulpitis of mature permanent teeth. MTA Pulpotomy can be used to treat acute irreversible pulpitis of an adult HIV-Positive patient alternative to root canal treatment as it is less invasive and one-step endodontic therapy.
Objective: The aim was to evaluate the outcome of MTA Pulpotomy alternative to root canal treatment to manage acute irreversible pulpitis of an adult HIV-positive patient.
Methods: Based on history, clinical and radiological examination the case was diagnosed as acute irreversible pulpitis on the mandibular left 2nd molar tooth in a patient who was HIV-positive and under treatment for 16 years. After anaesthetising and isolation with rubber dam coronal pulp was completely removed and MTA (Angelus, Brazil) was placed over the pulp chamber floor covering the canal orifices, and the rest of the cavity was sealed with glass-ionomer filling over the set MTA. The severity of postoperative pain was assessed by a visual analog scale after 24 hours, 48 hours, 72 hours, and 7 days. The incidence of any clinical symptoms or periapical pathology was determined using clinical and radiographic evaluation after 3-month, 6 months, and 1-year intervals.
Results: Throughout the follow-up period, the patient was asymptomatic and there was no periapical pathology at the radiograph even at the end of one year.
Conclusion: As a less invasive and single sitting short procedure, MTA pulpotomy can be done to treat acute irreversible pulpitis in the HIV-positive patient as an alternative to root canal treatment.Keywords: MTA pulpotomy, Acute irreversible pulpitis, HIV-positive patient, Root canal treatment.
Introduction
Approximately 1.1 million people are living with HIV.1 HIV-positive patient needs very careful dental management to avoid the risk of transmission of the disease. In case of any dental procedure for HIV- positive patients, it is better to choose any less invasive and less time-consuming procedure, if possible.
Acute irreversible pulpitis is a dental emergency that required early treatment to reduce the pain. In the case of acute irreversible pulpitis, the accepted treatment option is root canal treatment which is a more invasive and expensive procedure and sometimes multiple visits are necessary to complete the treatment. Another option is the extraction of the tooth, if a patient is not able economically to bear the expense of root canal treatment which is also a more invasive procedure and some laboratory tests and some extensive precautions are necessary to do the extraction. So, a less invasive treatment protocol for acute irreversible pulpitis is a crying need for the HIV- positive patient. Recently a new treatment option named pulpotomy procedure is considered effective and comparable to root canal treatment to treat acute irreversible pulpitis of mature permanent tooth. As this procedure is less invasive, less time consuming (single visit procedure), not expensive, and better for infection control, this alternative treatment was done to manage a case of acute irreversible pulpitis of an adult HIV-positive patient, and clinical and radiological evaluation was done at 3-month, 6 months and 1-year interval.
The Case
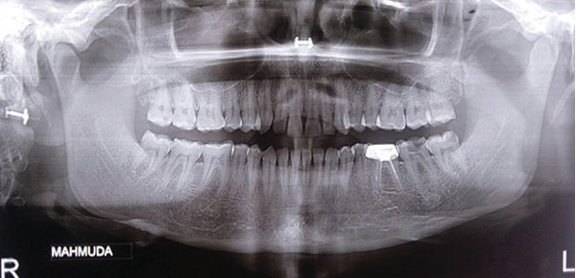
A 35-year old female patient came to the department of conservative dentistry and Endodontics with the complaint of pain on the lower left posterior jaw for 3 days. On clinical examination, there was a deep carious lesion on the lower left 2nd molar tooth (figure 1). (Figure 1). The pain was spontaneous but no swelling, sinus tract, tenderness to palpation, and percussion were present. The pain only reduced with NSAIDs. The normal probing depth and no mobility were present. The exaggerated and lingering response was present on the cold and heat test. More intense and early response at lower threshold was found at EPT. On radiographic examination, normal PDL space and intact lamina dura were found and there was no periapical radiolucency. Acute irreversible pulpitis on tooth no 37 was diagnosed based on history taking, clinical and radiological evaluation.
The patient’s medical history revealed diagnosed case of HIV positive by ELISA test followed by the Western Blot test 16 years ago. Now the patient is under follow up at a 6-month interval, at the HIV Corner of BSMMU, Dhaka, and the present CD4 count is consistently normal (Ã400 cells per microliter)
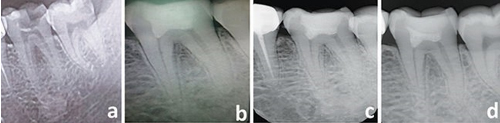
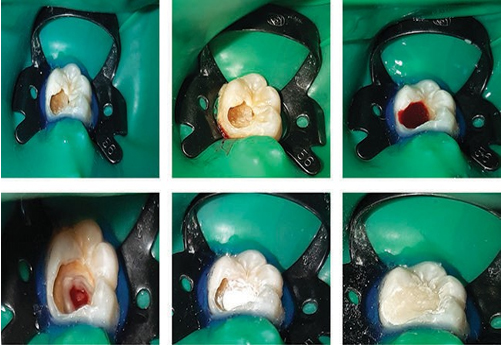
All aseptic precautions and standard protocol of infection control were taken before starting the pulpotomy procedure. The treatment protocol was similar to the standard pulpotomy procedures as suggested by Witherspoon et al.2 The tooth was anaesthetised using 2% lignocaine hydrochloride with epinephrine 1:80,000 (Jasocaine- A, Jayson Pharmaceuticals Ltd, Bangladesh), and isolated under a rubber dam (figure 3a) (Figure 3). The crown was disinfected with 5% NaOCl before caries excavation. The carious lesion was excavated using a large round diamond bur in a high-speed handpiece with water coolant and spoon excavators (figure 3b). Using another fresh sterile round bur, the pulp chamber was deroofed and the opening was refined with sterile tapered diamond bur (EndoAccess Bur; Dentsply Maillefer). During this time pulp vitality was confirmed by the presence of active bleeding pulp tissue after exposure of pulp (figure 3c). Coronal pulp tissue was excised using a spoon excavator until the canal orifice. Haemorrhage was controlled using a sterile cotton pellet moistened with normal saline applied for 2 to 3 minutes (figure 3d). After hemorrhage control, the chamber was cleaned using 5 mL 2.5% NaOCl, dried with sterile gauze or cotton pellet, and a freshly mixed paste (according to the manufacturer’s instructions) of white mineral trioxide aggregate (MTA) (Angelus; Brazil) was placed over the chamber floor covering the canal orifices (figure 3e). Then MTA (Angelus; Brazil) was condensed lightly with moistened cotton pellet to attain an adequate thickness of 2 to 4 mm confirmed radiographically. As the setting time of this type of MTA is only 15 minutes, therefore no need for a damped cotton pellet is placed over the condensed MTA and the cavity was sealed with Ketac Molar glass-ionomer filling (3M/ ESPE, Seefeld, Germany) over the set MTA after 15 minutes (figure 3f). Occlusal adjustment of the restoration was made, finished, and polished. A postoperative radiograph was taken for future comparisons. The severity of postoperative pain was assessed by a visual analog scale after 24 hours, 48 hours, 72 hours,and 7 days. After 48 hours there was no postoperative pain. The patient had clinical and radiographic evaluation after 3 months, 6 months, and 1-year postoperatively. Throughout the follow-up period and at the end of the 1-year patient was asymptomatic and the tooth was fully functional. No periapical pathology with normal PDL space was found on the radiograph (Figure 2).
Discussion
Pulpotomy has been considered as a definitive treatment to manage carious pulp exposure for primary teeth, young immature permanent teeth as well as in treating traumatic pulp exposure in mature teeth. In recent years, there have been a growing number of studies assessing clinical outcomes of Pulpotomy in mature permanent tooth.3-6
Histologic studies show that teeth with irreversibly damaged pulp, either symptomatic or asymptomatic, can exhibit the coexistence of the damaged and healthy pulp in the various parts of the total pulpal area.7 Therefore, a possibility lies that after the removal of pulp tissue that has undergone degenerative and irreversible changes, conservation of the remaining healthy pulp may be possible. This rationale has been supported in several clinical studies by the demonstration of the successful outcomes of pulpotomy.8,9
Using coronal pulpotomy treatment, proper case selection and treatment protocols are essential if it is to be successful.11 Teeth exhibiting symptoms suggestive of irreversible pulpitis have little chance to revert to normal if no other intervention takes place than removal of irritants. In these cases, the section of the pulp that is inflamed must be removed so that the remaining uninflamed tissue can recover and heal.7 This has proven to be successful, both in histological and clinical studies and teeth diagnosed with irreversible pulpitis have been successfully treated with a pulpotomy.8,10,11 Compared to RCT, Pulpotomy is a less technique sensitive that can be performed by general dental practitioners, particularly for treating posterior permanent teeth. Hence, pulpotomy may increase patients’ access to dental care and more clinicians would be able to provide this affordable procedure when the patients’ finances prohibit RCT, leaving only extraction as a treatment option.14
In cases of acute pulpitis, endodontic treatment must be performed immediately to eliminate the risk of periapical infection and other complications. When patients with medical conditions like HIV infections or AIDS are unable to return for repeated appointments, one-step endodontic therapy should always be considered.13 Pulpotomy seems very favorable endodontic therapy for treating acute irreversible pulpitis of an HIV-positive patient as it can be done single sitting while root canal treatment can’t be done in single visit always and sometimes multivisit appointment is required.
HIV targets a particular form of immune cell in the human body. It’s also known as a T cell or CD4 helper cell.1 When HIV kills this cell, the body’s ability to fend off other infections is harmed. An individual has advanced to AIDS when the virus has killed a certain number of CD4 cells and the CD4 count falls below 200. In a study MTA showed no cytotoxic effect on the adaptive immune cells16 and the application of MTA is considered highly effective as it does not compromise either innate or adaptive immune response.17 On the other hand MTA stimulates new hard tissue formation and promotes pulp repair.12,15 Thicker dentinal bridges are formed and the presence of an odontoblastic layer was reported in histological evaluation of teeth restored with MTA.15
Conclusion
MTA pulpotomy treatment was found successful as an alternative to root canal treatment to treat acute irreversible pulpitis in the immunocompromised condition of a patient like HIV infection.
References
- Burgess J. HIV and Dental Treatment. JSM Dent. 2016; 4:1062.
URL: www.jscimedcentral.com/Dentistry/dentistry-4-1062.pdf - Witherspoon DE, Small JC, Harris GZ. Mineral trioxide aggregate pulpotomies: a case series outcomes assessment. J Am Dent Assoc. 2006; 137:610–8.
DOI: 10.14219/jada.archive.2006.0256 - Simon S, Perard M, Zanini M, Smith AJ, Charpentier E, Djole SX, Lumley PJ. Should pulp chamber pulpotomy be seen as a permanent treatment? Some preliminary thoughts. Int Endod J. 2013; 46:79-87.
DOI: 10.1111/j.1365-2591.2012.02113.x - Kunert GG, Kunert IR, da Costa Filho LC, de Figueiredo JAP. Permanent teeth pulpotomy survival analysis: retrospective follow-up. J Dent. 2015; 43:1125-31.
DOI: 10.1016/j.jdent.2015.06.010 - Asgary S, Fazlyab M, Sabbagh S, Eghbal MJ. Outcomes of different vital pulp therapy techniques on symptomatic permanent teeth: a case series. Iran Endod J. 2014; 9:295- 300
PMID: 25386213 - Alqaderi H, Lee CT, Borzangy S, Pagonis TC. Coronal pulpotomy for cariously exposed permanent posterior teeth with closed apices: A systematic review and meta-analysis. J Dent. 2016; 44:1-7.
DOI: 10.1016/j.jdent.2015.12.005. - Ricucci D, Loghin S, Siqueira JF Jr. Correlation between clinical and histologic pulp diagnoses. J Endod. 2014; 40:1932-9.
DOI: 10.1016/j.joen.2014.08.010 - Qudeimat MA, Alyahya A, Hasan AA. Mineral trioxide aggregate pulpotomy for permanent molars with clinical signs indicative of irreversible pulpitis: a preliminary study. Int Endod J. 2017; 50:126-134.
DOI: 10.1111/iej.12614. - Galani M, Tewari S, Sangwan P, Mittal S, Kumar V, Duhan J. Comparative Evaluation of Postoperative Pain and Success Rate after Pulpotomy and Root Canal Treatment in Cariously Exposed Mature Permanent Molars: A Randomized Controlled Trial. J Endod. 2017; 43:1953-1962.
DOI: 10.1016/j.joen.2017.08.007 - Solomon RV, Faizuddin U, Karunakar P, Deepthi Sarvani G, Sree Soumya S. Coronal Pulpotomy Technique Analysis as an Alternative to Pulpectomy for Preserving the Tooth Vitality, in the Context of Tissue Regeneration: A Correlated Clinical Study across 4 Adult Permanent Molars. Case Rep Dent. 2015; 2015:916060.
DOI: 10.1155/2015/916060. - Taha NA, Ahmad MB, Ghanim A. Assessment of Mineral Trioxide Aggregate pulpotomy in mature permanent teeth with carious exposures. Int Endod J. 2017; 50:117-125.
DOI: 10.1111/iej.12605 - Parirokh M, Torabinejad M, Dummer PMH. Mineral trioxide aggregate and other bioactive endodontic cements: an updated overview - part I: vital pulp therapy. Int Endod J. 2018; 51:177-205.
DOI: 10.1111/iej.12841 - Abel SN, Croser D, Fischman SL, Glick M, Phelan JA. Principles of Oral Health Management for the HIV/AIDS Patient, 2000 edition. Dental Alliance for AIDS/HIV Care (DAAC).
URL: resources_files/Princ_Oral_Health_HIV.pdf - Alqaderi HE, Al-Mutawa SA, Qudeimat MA. MTA pulpotomy as an alternative to root canal treatment in children’s permanent teeth in a dental public health setting. J Dent. 2014; 42:1390-5.
DOI: 10.1016/j.jdent.2014.06.007 - Aeinehchi M, Eslami B, Ghanbariha M, Saffar AS. Mineral trioxide aggregate (MTA) and calcium hydroxide as pulp- capping agents in human teeth: a preliminary report. Int Endod J. 2003; 36:225-31.
DOI: 10.1046/j.1365-2591.2003.00652.x. - Rezende TM, Vieira LQ, Sobrinho AP, Oliveira RR, Taubman MA, Kawai T. The influence of mineral trioxide aggregate on adaptive immune responses to endodontic pathogens in mice. J Endod. 2008; 34:1066-71.
DOI: 10.1016/j.joen.2008.06.006. - Yuan Z, Zhu X, Li Y, Yan P, Jiang H. Influence of iRoot SP and mineral trioxide aggregate on the activation and polarization of macrophages induced by lipopolysaccharide. BMC Oral Health. 2018; 18:56.
DOI: 10.1186/s12903-018-0511-9.
Department of Conservative Dentistry, Sir Salimullah Medical College Dental Unit, Dhaka, Bangladesh.
imran.v.2022@gmail.com
 0000-0002-6218-2263
0000-0002-6218-2263
Submission
2021-05-12
Accepted
2021-06-30
Published
2021-08-01
Apply citation style format of Bangladesh Medical Research Council
Issue
Vol 47 No 2 (2021)
Section
Case Report
Financial Support
None
Conflict of Interest
None