Mahbuba Akhter
Department of Physiology, Chittagong Medical College, Chattogram, Bangladesh.
Momtaz Begum
Department of Physiology, Chittagong Medical College, Chattogram, Bangladesh.
Shahin Akhter
Department of Physiology, Chittagong Medical College, Chattogram, Bangladesh.
Arunima Datta
Sunamganj Sadar Hospital, Sunamganj, Bangladesh.
Nazrul Islam
Upazila Health Complex, Begumgonj, Noakhali, Bangladesh.
Raju Chowdhury
Department. of Anatomy, North East Medical College, Sylhet, Bangladesh.
Keywords: Cement, Pulmonary function, Spirometer, Forced vital capacity.
DOI: 10.3329/bmrcb.v47i2.57780
Abstract
Background: Cement industries are playing a key role in economic growth and infrastructure development. But its production is a dusty process and is a major source of air pollution. Its exposure may affect respiratory system and impairment of pulmonary functions.
Objective: This study was aimed to assess the effects of cement dust on pulmonary functions of workers working in cement factory.
Methods: This case control study was conducted in the department of physiology, Chittagong Medical College, Chattogram in collaboration with Heidelberg Cement Bangladesh Ltd. in Chattogram from January 2018 to December 2018. A total of 88 male workers, aged between 20-45 years were included in this study by consecutive sampling method who met the inclusion criteria. Workers working at least two years in direct contact of cement dust were considered as exposed (case) group. Non exposed (control) group were selected from office workers of same factory those who were not directly exposed to cement. Each group included 44 subjects. A predesigned data collection form containing information regarding general information, job history, present and past disease, drug history was filled up. Individual’s height, weight was measured and BMI was calculated. FVC, FEV1, FEV1/FVC (%) was recorded by a digital spirometer (Chestgraph HI-101, Japan) in upright sitting posture. After compiling data,statistical analyses were done by using SPSS version Windows 25. Unpaired student’s ‘t’ test was done for statistical analysis.
Results: Exposed (case) group showed significant reduction of FVC and FEV1 (p<0.001)with unaltered FEV1/ FVC (%) (p>0.05) in comparison to non exposed (control) group.
Conclusion: The results of this study concluded that occupational exposure to cement dust reduce pulmonary functions of cement workers.
Keywords: Cement, Pulmonary function, Spirometer, Forced vital capacity.
Introduction
Development of this modern world markedly depends on cement industry due to rapid urbanization and industrialization.1 Cement is a major construction material that is used for housing and infrastructure development.1 As this industry creates employment and business opportunities for people, millions of people are engaged in this sector.2,3
But the cement manufacturing projects are considered as major source of air pollution due to different hazardous emissions.1 This industry is the third largest source of air pollution.2 Occupational airborne diseases are considered as one of the important cause of death and disabilityamong people.4 Per year about 386000 deaths occur due to exposure of airborne particles.4
Cement is a light gray powder which diameter is ranged between 0.05 to 5.0 µm.5,6 Two types of cement are available – natural and artificial.2 Artificial cement is known as Portland cement which is a mixture of oxides of Calcium (CaO) (61-67%), Silicon (SiO2) (19-23%), Aluminium (Al2O3) (3-6%), Iron (Fe2O3) (2-6%), Magnesium (MgO) (1-2%), Selenium, Thallium and some other impurities.6 Major pollutants contained in cement are Nitrogen oxide (NOx), Sulfur dioxide (SO2) and Carbon monoxide (CO).2 SO2 May cause throat and nose irritation, Nitrogen oxide may cause lung tissue damage and CO can cause reduction of Oxygen delivery to various organs and tissues.2 It may also contribute to smog formation in air which create respiratory problems.2
Long term exposure of cement dust may cause varying degree of lung function reduction, respiratory symptoms like dyspnea, chest pain, sneezing, phlegm, wheeze, prolonged and recurrent cough, pneumoconiosis, bronchitis, sinusitis, bronchial asthma and lung cancer.2,6-9
Cement dust particles may enter through respiratory tract or gastrointestinal tract or both by inhalation or swallowing.8 Health risk on people depends on deposition pattern, exposure duration, size and composition of the particles, individual susceptibility and biological responses exerted by particles in various region of respiratory tract.1,10-11
Though millions of people are engaged with this industry but most of them are unaware of hazardous effect of cement on human body.12 So, they work without proper protective equipment, high quality face mask, appropriate training and inadequate knowledge regarding their working environment.12 Several previous study observed pulmonary function test like FVC, FEV1 and FEV1/FVC (%) of cement workers by spirometer to observe the effect of cement on pulmonary functions.5-7,13-16 Some researchers found significant reduction, some found unaltered lung function in their study subjects.5-7,13-16 In Bangladesh, no adequate data is available regarding the effect of cement dust on pulmonary functions. So, this study was designed to evaluate the effect of cement dust on pulmonary functions such as forced vital capacity (FVC), forced expiratory volume in 1st second (FEV1) and FEV1/ FVC (%) to make awareness and protect the workers from developing chronic respiratory disease, which may be also helpful for lowering medical costing of the workers and development of economic growth of the country.
Materials and Methods
This case control study was conducted in the department of physiology,Chittagong Medical College, Chattogram with collaboration of Heidelberg Cement Bangladesh Ltd. Chattogramfrom January 2018 to December 2018. Ethical approval was obtained from the IRB of the Chittagong Medical College. Study subjects were selected from workers of Heidelberg cement factory ltd. at Chattogram. Forty four apparently healthy, 20-45 yearsaged non-smoker male, working 8-10 hrs/day for six days/week for more than 2 years in direct contact of cement were selected as exposed (case) group.Age matched non exposed (control) group were taken from office workers of same factory those who were not in direct contact of cement dust. They were explained about the aims, objectives and whole procedure of the study clearly. They were also encouraged for voluntary participation and allowed freedom to withdraw from the study at any time. They were also ensured that collected data will be used only for research purpose. Informed written consent was taken from each individual.
On the basis of inclusion and exclusion criteria subjects were selected by consecutive sampling method. On the day of data collection information of subjects regarding age, job duration, site and position of work place, use of safety gadget,physical condition, drug and smoking history, acute or chronic cardiorespiratory abnormality of subjects were recorded. Subjects having history of any respiratory disease, skin rash, chronic cough, fever, acute infection, hypertension, chest deformities, history of major abdominal or thoracic surgery, diabetes, hypertension, those who were taking bronchodilators, sedative, antitubercular therapy, steroid, beta blocker, chemotherapeutics were excluded from the study.
Height was measured in feet-inches by plotting a height measuring scale against the wall. Standing straightly on bare foot, from the top of the vertex to the bottom of the foot height was recorded.Weight was measured in kilogram (Kg) by a standard analogue weighing machine on bare foot and avoid excess clothing. Then BMI was calculated general physical examination was performed.
For exclusion of diabetes mellitus RBS was measured by glucometer (One touch ultra, USA, A W-061-566-01A) and to exclude anaemia Hb% was done instantaneously by Sahli-Adam’s acid hematin method with the help of a trained technician.
After analysing the case record form, selected subjects were undergone spirometry. Prior to spirometry, they were demonstrated clearly and practiced several times. Those who performed perfectly were included as study subject.
For spirometric test subjects were asked to sit upright on a comfortable chair quietly with loose clothing and relaxed for 5 minutes. Then switch of the spirometer was on and information regarding subject’s ID, age, height (cm), weight (kg), sex, race was imputed in the device. Disposable card board mouthpiece was used for each individual.After nose clipping, mouthpiece was placed in between the lips of subject.17 They were asked to hold the mouthpiece horizontally in their hand and put the lips tightly around the mouthpiece for good sealing. Then they were asked to inhale as deeply and rapidly as possible and exhale forcefully as possible for possible longest period into the mouthpiece.17 After three attempts, the best of three recordings was taken. Then nose clips were removed andthe machine was powered off.17 The readings of FVC, FEV1, FEV1/FVC (%) were collected from the tracing of spirometer and recordedin data collection form.
After compiling data were analysed by using SPSS (Statistical Program for the Social Sciences) version on 25. Between groups comparison of variables were done by unpaired student’s ‘t’ test. p value <0.05 was accepted as level of significance.
Results
The mean (± SD) age of non exposed (control) group and exposed (case) group were 37.05±6.52 years and 37.23±8.29 years respectively.The mean (± SD) height of non exposed (control) group and exposed (case) group were 164.89±4.68 cm and 164.50±3.91 cm respectively. The mean (±SD) weight of non exposed (control) group and exposed (case) group were60.18±3.71 kg and 60.02±3.55 kg respectively. The mean (± SD) BMI of non exposed (control) group and exposed (case) group were 22.10±0.88 kg/m2 and 22.17±0.73 kg/m2 (table I). Non significant difference (p>0.05) were observed regarding age, height, weight and BMI of both group workers (table I).
Variables |
Non exposed Group (control) [n=44] Mean ± SD (Range) |
Exposed Group (case) [n=44] Mean ± SD (Range) |
p value (t value) |
|---|---|---|---|
Age (years) |
37.05 ± 6.52 |
37.23 ± 8.29 |
0.909ns |
|
(22 - 45) |
(21 - 45) |
(0.114) |
Height (cm) |
164.89 ± 4.68 |
164.50 ± 3.91 |
0.675ns |
|
(152 - 172) |
(157 - 172) |
(0.420) |
Weight (Kg) |
60.18 ± 3.71 |
60.02 ± 3.55 |
0.837ns |
|
(52 - 68) |
(52 - 68) |
(0.206) |
BMI (Kg/m2) |
22.10 ± 0.88 |
22.17 ± 0.73 |
0.713ns |
|
(19.70 – 22.90) |
(20.10 – 22.90) |
(0.369) |
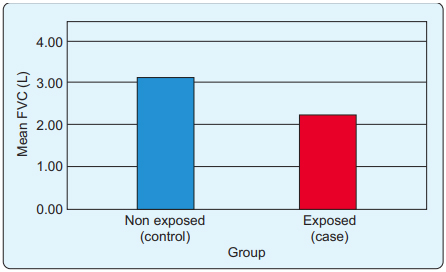
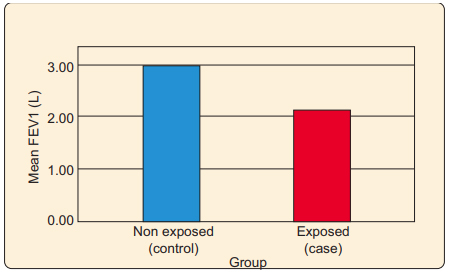
Mean (± SD) FVC of non exposed (control) group and exposed (case) group were 3.13±0.37 liter and 2.22±0.30 liter respectively.Mean (± SD) FEV1 of non exposed (control) group and exposed (case) group were 2.97±0.33 liter and 2.13±0.28 liter respectively. Mean (± SD) FEV1/FVC (%) of non exposed (control) group and exposed (case) group were 95.01±5.35 % and 95.82±5.23% respectively (table II).
The mean of FVC and FEV1 was significantly (p<0.001) reduced in exposed (case) group workers (Table II). Bar charts also showing the difference between two groups regarding FVC and FEV1 (Figure 1 and Figure 2). But FEV1/FVC (%) showed non significant (p>0.05) difference in both group (table II).
Variables |
Non exposed group (control) [n=44] Mean ± SD (Range) |
Exposed group (case) [n=44] Mean ± SD (Range) |
p value (t value) |
|---|---|---|---|
FVC (Liter) |
3.13 ± 0.37 |
2.22 ±0.30 |
<0.001** |
|
(2.53 – 3.91) |
(1.70 – 2.86) |
(12.61) |
FEV1 (Liter) |
2.97 ± 0.33 |
2.13 ± 0.28 |
<0.001** |
|
(2.38 – 3.67) |
(1.58 – 2.78) |
(12.72) |
FEV1/FVC (%) |
95.01 ± 5.35 |
95.82 ± 5.23 |
0.473ns |
|
(80.40 – 100) |
(81.45 – 100) |
(0.721) |
**= statistically significant test (p<0.001), ns = not significant (p>0.05)
Discussion
In this study, no significant difference was observed between non exposed (control) and exposed (case) group workers in respect of age, height, weight and BMI. It indicates that subject selection was similar in both group.
Pulmonary functions FVC and FEV1 showed significant reduction among exposed (case) group workers in comparison to non exposed (control) group workers. But FEV1/FVC (%) showed insignificant difference. This study finding simulate with some previous studies done by other researchers.5,7,13-15, 18It was supposed that, as cement dust contain chromium and silica which act as foreign particle, accumulated in respiratory tract may cause lung irritation and inflammation with mucus hypersecretion.9,12,16,19 Some researcher supposed that, due to inflammation Histamine and Serotonin is released from degranulated amines.9 So, bronchial smooth muscles and vascular endothelium are affected and produces symptoms of atopic condition.9 Dust particles sized 3µm-10µm can deposited in tracheobronchial tree and <3µm can be deposited in alveoliand produce clinical presentation.3 As cement dust particle size is within respireable range, it produces respiratory sign symptoms and pulmonary function impairment.
Occupational health risk influenced by some factors like duration of dust exposure, deposition pattern, chemical composition, size and concentration of dust particles.1,5,12 According to Environment Conservation Rules; 1997, in Bangladesh the level of suspended particulate matter (SPM) are fixed at below 200µg/m3.20 Butthe research work carried out in which factory, SPM was 230 µg/m3, which is slightly more than the recommended level for our country.
Some researchers proposed that pulmonary function reductionmight be due to inadequate dust control system, overtime duty, improper use of personal protective equipment (PPE).10,13,21 In this study, it was observed that the workers were using PPE though they used non medicated cotton face mask. So, in this study FVC, FEV1 reduction among exposed (case) group may be due to their inappropriate and interrupted use of PPE or poor quality facemaskused by the workers. Inadequate dust filtration system of that factory may be also responsible for pulmonary function impairment.
Non significant difference regarding FEV1/FVC (%) may be due proportionate reduction of both FVC and FEV1 of exposed (case) workers.22 It was also supposed that unaltered FEV1/FVC (%)may be due to restrictive type lung function impairment.5,7,14,23 As x-ray chest or surface electromyography of the workers were not done, so it was not confirmed that the study subjects had restrictive type lung function impairment or not. Study done by Meo SA et al. in 2002 suggested that reduced lung and chest wall compliance among dust exposed workers might be responsible for restrictive changes in lung.22 It was confirmed by impairment of intercostal muscle performance by surface electromyography (SEMG)in that study.22
Some study findings dissimulate with this study result. Sumana PV et al in 2016 and Rafeemanesh E et al. in 2015 was observed insignificant change of pulmonary functions among cement exposed worker.6,16 They supposed that the use of personal protective equipment by the workers under strict supervision and dust exposure level within threshold limit in their working area may responsible for insignificant impairment.6,24
This study result suggested that exposure to cement dust affect respiratory system and progressive lung function impairment of workers. If pre-employment and periodic health checkup at least once in a year can be ensured, the further impairment can be reduced and productivity of the workers can be increased.
Conclusion
This study result concluded that cement dust exposure significantly reduced pulmonary functions. Though exact mechanism is not known behind this reduction but it may be due to their improper dust filtration system or ineffective personal protective equipment by the workers and unawareness about the health risk related to cement.If further study can be done with large sample size, individual dust exposure level measurement and chest x-ray, it may provide more accurate result.
Acknowledgments
The authors acknowledge the support of study subjects and authority of Heidelberg Cement Factory Bangladesh Ltd. Chattogram and Department of Physiology, CMC, Chattogram for giving the permission and laboratory instrument uses.
References
- Aljeesh Y, Madhoun WA, Jabaly EI. Effect of exposure to cement dust on pulmonary function among cement plants workers in the middle Governorate, Gaza, Palestine. Public Health Research. 2015;5:129-34.
DOI: 10.5923/j.phr.20150505.01 - Rampuri S. Study and analysis of occupational and health diseases in cement industries. International Journal of Advance Research and Development. 2017;2:1-7.
Available from: www.ijarnd.com/manuscripts/v2i3/V2I3-1139.pdf - Manjula R, Praveena R, Clevin RR, Ghattargi CH, Dorle AS, Lalitha DH. Effects of occupational dust exposure on the health status of Portland cement factory worker. International Journal of Medicine and Public health. 2013;3:192-96.
DOI: 10.4103/2230-8598.118963 - Driscoll T, Nelson DI, Steenland K, Leigh J, Barrientos MC, Fingerhut M et al. The global burden of non-malignant respiratory disease due to occupational airborne exposures. American Journal of Industrial Medicine. 2005:1-17.
Available from: www.who.int/quantifying_ehimpacts/global/4airbornexposure.pdf - Mirzaee R, Kebriaei A, Hashemi SR, Sadeghi M, Shahrakipour M. Effects of exposure to portland cement dust on lung function in portland cement factory workers in Khash, Iran.Iran. Journal of Environmental Health Science and Engineering. 2008;5:201-6.
Available from: www.researchgate.net/publication/26518952 - Rafeemanesh E, Alizadeh A, Saleh LA, Zakeri H.A study on respiratory problems and pulmonary function indexes among cement industry workers in Mashhad, Iran. Medycyna Pracy. 2015;66:471–77.
Available from: www.researchgate.net/publication/26518952 - Badri OAEI, Saeed AM. Effect of exposure to cement dust on lung function of workers at Atbara cement factory. Kharoum Medical Journal. 2008;1:81-84.
Available from: www.researchgate.net/publication/277214382 - Siyoum K, Alemu K, Kifle M. Respiratory symptoms and associated factors among cement factory workers and civil servants in North Shoa, Oromia Regional State, North West Ethopia: comparative cross sectional study. Occupational Medicine and Health Affairs. 2014;2:1-8.
DOI: 10.4172/2329-6879.1000182 - Richard EE, Chinyere NAA, Jeremaiah OS, Opara UCA, Henrieta EM, Ifunanya ED. Cement dust exposure and perturbations in some elements and lung and liver functions of cement factory workers. Journal of Toxicology. 2016:1-7.
DOI: 10.1155/2016/6104719 - Zeleke ZK, Moen BE, Bratveit M. Cement dust exposure and acute lung function: A cross shift study. BMC Pulmonary Medicine. 2010;10:1-8.
DOI: 10.1186/1471-2466-10-19 - Dawood HN, Larazak ARMA, Muhasen AM. Pulmonary function test in cement workers in Iraq. The Iraqi Postgraduate Medical Journal. 2013;12:85-89.
Available from: www.iasj.net/iasj/download/ab9937f211cac009 - Aminian O, Aslani M, Haghighi KS. Cross-shift study of acute respiratory effects in cement production workers. Acta Medica Iranica. 2014;52:146-52.
Available from: www.researchgate.net/publication/261034389 - Vyas S. A study of pulmonary function tests in workers of different dust industries.International Journal of Basic and Applied Medical Sciences.2012;2:15-21.
Available from: www.cibtech.org/J-MEDICAL- SCIENCES/PUBLICATIONS/2012/JMS-02-02/02...003%20Sangeeta% 20Vyas...A% 20Study%20 of...Industries...pdf - Neghab M, Choobineh A.Work- related respiratory symptoms and ventilatory disorders among employees of a cement industry in Shiraz, Iran. Journal of Occupational Health. 2007;49:273-78.
DOI: 10.1539/joh.49.273 - Paranjape A. A study on effect of cement dust on pulmonary function test in construction workers. Walawalkar International Medical Journal. 2018;5:26-32.
Available from: www.doi-ds.org/doilink/08.2018-59789427/ - Sumana P V, Jemima M, Rani D, Madhuri T. Cement dust exposure and pulmonary function tests in construction site workers.Asian Pacific Journal of Health Sciences. 2016;3:43-46.
DOI: 10.21276/apjhs.2016.3.2.9 - Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A et al. Standardisation of spirometry. European Respiratory Journal. 2005; 26: 319-38.
DOI: 10.1183/09031936.05.00034805 - Meo SA, Al-Drees AM, Al Masri AA, Al Rouq F, Azeem MA. Effect of duration of exposure to cement dust on respiratory function of non-smoking cement mill workers. International Journal of Environmental Research and Public Health. 2013;10:390-98.
DOI: 10.3390/ijerph10010390 - Ashwini S, Swathi K, Saheb SH.Effects of cement dust on pulmonary function test parameters. Acta Biomedica Scientia. 2015;3:71-74.
Available from: www.researchgate.net/publication/290432172 - Environment Conservation Rules-1997. [Internet] [cited 2021 Jan 12].
Available from: www.scribd.com/document/55948700/Environment-Conservation-Rules,1997 - Al-Neaimi YI, Gomes J. and Lioyd OL. Respiratory illness and ventilatory function among workers at a cement factory in a rapidly developing country. Occupational Medicine 2001;51:367-73.
DOI: 10.1093/occmed/51.6.367 - Meo SA, Azeem MA, Ghori MG, Subhan MMF. Lung function and surface electromyography of intercostal muscles in cement mill workers. International Journal of Occupational Medicine and Environmental Health. 2002;15:279-87.
DOI: www.researchgate.net/publication/11009180 - Kakooei H, Gholam A, Ghasemkhani M, Hosseini M, Panahi D, Pouryaghoub G. Dust exposure and respiratory health effects in cement production. Acta Medica Iranica. 2012;5:122-26.
Available from: www.researchgate.net/publication/221855590 - Fell AKM, Thomassen TR, Kristensen P, Egeland T, Kongerud J. Respiratory symptoms and ventilatory function in workers exposed to Portland cement dust. Journal of Occupational and Environmental Medicine. 2003;45:1008-14.
DOI: 10.1097/01.jom.0000083036.56116.9d
Department of Physiology, Chittagong Medical College, Chattogram, Bangladesh.
msharmin2012@gmail.com
 0000-0002-3496-5949
0000-0002-3496-5949
Submission
25 February 2021
Accepted
30 June 2021
Published
01 August 2021
Apply citation style format of Bangladesh Medical Research Council
Issue
Vol 47 No 2 (2021)
Section
Research Articles
Ethical Clearance
IRB of Chittagong Medical College, Bnagladesh.
Financial Support
None.
Conflict of Interest
The authors declare no conflict of interest.