Khursheda Akhtar
National Institute of Preventive and Social Medicine, Bangladesh.
Kazi Jahangir Hossain
Shaheed Monsur Ali Medical College, Uttara, Dhaka, Bangladesh.
Shamsun Nahar
Department of Oncology, Bangabondu Sheikh Mujib Medical University, Dhaka, Bangladesh.
Khodeza Akhtar
Department of Conservative Dentistry, Chittagong Medical College, Chattogram, Bangladesh.
Keywords: Laboratory diagnosis, Diagnosis delay, Breast cancer, Fine needle aspiration cytology.
DOI: 10.3329/bmrcb.v47i2.57771
Abstract
Background: Diagnosis is a key determinant for any disease outcome. For that, we want to find out in which stage a breast cancer patient got admitted in hospital including various methods of laboratory investigations were done at different visits.
Objectives: This study was aimed to generate information on the stages that a breast cancer patient got admitted including various methods of laboratory investigations were done at different visits.
Methodology: We conducted a cross sectional study at the National Institute of Cancer Research and Hospital, Dhaka, Bangladesh from July 2017-June 2018. We randomly selected a total of 200 patients who came to that hospital through face-to-face interview by using pretested semi-structured questionnaire.
Results: A total 77.0% (154) patients investigated Fine Needle Aspiration Cytology (FNAC) at first visit and mean duration for diagnosis was 11 months. Maximum patients came for diagnosis at stage II, III or IV; nobody came at stage I. As consequences, we found that stage of cancer had 7 times more likely to cause diagnostic delay (OR=7.957; 95% CI 3.206-19.749) p <0.0001. Number of consultations was one of the cause for diagnostic delay (X2= 12.825, p <0.0001). Diagnostic delay had strong association between first consultation with physician versus other health care providers (X2= 17.645, p <0.0001). Excluding physicians, first consultation with health care providers also had 3 times more likely to cause delay in diagnosis (OR-3.862; 95% CI1.877-7.944) p<0.0001.
Conclusion: Breast cancer patients attended to health care provider at advanced stage. Knowledge, negative perception, social support were the contributing factor for delay in breast cancer diagnosis.
Keywords: Laboratory diagnosis, Diagnosis delay, Breast cancer, Fine needle aspiration cytology.
Introduction
Diagnosis of a disease is a complex process of determining and correspond which disease or condition explains a person’s symptom and sign. Breast cancer get bigger public health problem all over the world, especially in developing regions, where the incidence is growing as much as five percent per year.1,2 Each year, breast cancer is newly diagnosed in more than 1 million women worldwide with more than 400,000 women die from it.1,3 Though in Bangladesh, there is no national cancer registry but it is predicted that it will be an increasingly important cause of morbidity and mortality in the next few decades.6 Bureau of Statistics of Bangladesh stated that, cancer is the sixth leading cause of death. The estimated incidence of 12.7 million new cancer cases projected to 21.4 million by 2030. International Agency for Research on Cancer has estimated cancer-related death rates in Bangladesh to be 7.5% in 2005 and 13% in 2030.6
Diagnosis of a disease has a pivotal role to start cancer treatment. Maximum diagnosis of breast cancer usually done at advanced stage which leads to delay in starting breast cancer treatment. Delay diagnosis of breast cancer represents a significant problem in Bangladesh. It influences the survival rate and out pocket expenditure simultaneously. As cancer is a non communicable disease, more than two third of total expenditure is throughout pocket payments.6 Diagnosis of breast cancer is often challenging. False negative mammography or FNAC7 also has a pessimistic impact on cost and choice of treatment.7 The process of diagnosis may seem long and frustrating because, first patient and family member agree that it is a problem to seek medical help and visit health care provider. After that, physician correlates with physical finding by clinical examination and laboratory finding. If expected laboratory finding not matched with clinical examination or patient complain, repeated lab investigation is done. In Bangladesh, around one fourth respondents did not know to whom first seek help for breast cancer diagnosis and treatment.8
Delayed detection of breast cancer increases the chance of metastases as well mortality and morbidity. Early detection of cancer is important because delay is preventable and earlier treatment can lead to improved survival. To the best of our knowledge, no study has been previously conducted in Bangladesh to assess the diagnostic delay. Limited studies have been conducted in South East Asian.9-13
This study was conducted to generate information on the stages that a breast cancer patient got admitted including various methods of laboratory investigations were done at different visits to determine the duration required for breast cancer as well to whom and in which institution they go first, how many visits required and also to find out the factors related to the diagnostic delay.
Materials and Methods
A cross sectional study was conducted during July 2017-June 2018 with a total of 200 samples which were selected randomly from the National Institute of Cancer Research and Hospital, Dhaka, Bangladesh from the listed patients who attended in the outpatient department of chemotherapy day care centre for treatment after diagnosis of breast cancer. To avoid recall bias newly diagnosed primary carcinoma (breast cancer) patients were selected. Inclusion criteria were diagnosed breast cancer patients irrespective of age, marital status, education, religion and customs, admitted in the hospital and patients of breast cancer who was provided informed written consent. Patients with mental disability; seriously ill recurrence of breast cancer, treatment failure with metastasis; hearing impairment; and patients who were not provided informed written consent were excluded from the study. Patients were randomly approached and perspectives of the study were explained to the respondents and all eligible patients signed the consent forms before a face to face interview was conducted. Though sample size was calculated as 384 (p=49.1%14, z=1.96, d=0.05) but based on the exclusion criteria, in total 200 patients (52%) completed the interview. The reasons for non completion included the patients being too tired, having poor physical health, lack of interest. Each breast cancer patient was given chemotherapy at 21 days cycle. Daily approximately 7 breast cancer patients came for chemotherapy from different parts of the country. The interview was taken to 40 - 45 minutes in length. Ethical Clearance was obtained from Institutional Review Board (IRB) of NIPSOM (NIPSOM/IRB/2016/18) and written permission was obtained from hospital authority before taking interviews (NICRH/Ethics/2016/204-5). Written informed consent was obtained from all patients who participated in this study in a predesigned consent form. The questionnaire included questions focusing on patient’s socio demographic, current treatment status, factor related to diagnostic delay, medical help seeking for diagnosis and treatment. Clinical information such as stage of disease, type of surgical management etc were obtained from medical records. Questionnaire was prepared by reviewing literatures of qualitative study which was done in South East Asian Region and from various models.9-13,15, 16
Statistical analysis
Statistical analyses of the data were performed using the Statistical Package for the Social Sciences (SPSS) for Windows, version 23.0 (SPSS Inc.; Chicago, IL, USA). Descriptive statistics like frequency distribution, mean, median, mode, range, standard deviation etc. were calculated by SPSS programme. Association was seen between diagnostic time and other variables by Pearson’s Chi-square (X2) 2x2 table at p<0.05 level of significance. To control confounder logistic regression was done.
Results
Out of 200 respondents, maximum patients 77(38.5%) were in 36-45 age group and their mean age was 42 years with mean family income was around BDT 9000 (just over 100$). A total 154 (77 %) patients did FNAC for the first visit. FNAC was ahead one time done by 133 (66.5 %) respondents, two times was done by 56 (28%) and three times by only 6 (3%) respondents. Maximum were diagnosed in at stage III 130 (65.5%) and stage IV 32 (16.0%), only 38 (19%) respondents were in stage II (table-1).
Variables |
Number (Percentage) |
|---|---|
Age during first detection of symptom |
|
26-35 |
56 (28.0) |
36-45 |
77(38.5) |
Above 45 |
67(33.5) |
Mean ±SD ;42±9 |
|
Average monthly family income* (in taka) |
|
1000-5000 |
80(40.0) |
6000-10000 |
84(42.0) |
>10000 taka |
36(18.0) |
Mean family income in taka 8937± 880 |
|
*100$=8000 taka(approximately) |
|
Fine-Needle Aspiration Cytology ( FNAC) on first visit |
|
Yes |
154(77.0) |
No |
41(20.5) |
Never done |
5(2.5) |
Frequency of Fine-Needle Aspiration Cytology |
|
( FNAC) for breast cancer diagnosis |
|
One time |
133(66.5) |
Two times |
56(28.0) |
Three time |
6(3.0) |
Never done |
5(2.5) |
Time to breast cancer diagnosis (in months) |
|
1-6 |
71(30.5) |
7-12 |
60(30.0) |
More than 12 months |
69(34.5) |
Minimum=1,Maximum=48, Mean±SD;11±8.6 |
|
First diagnostic institution |
|
Private Hospital |
140(70.0) |
Public Hospital ( Medical College and District Hospital) |
43(21.5) |
Cancer Hospital |
17(8.5) |
Stage of breast cancer |
|
Stage I |
0(0.0) |
Stage II |
38(19.0) |
Stage III |
130(65.0) |
Stage IV |
32(16.0) |
First contact with health care providers for diagnosis |
|
Homeopathy |
95(47.5) |
Post graduate physician |
67(33.5) |
MBBS* physician |
38(19.0) |
Number of consultation(s) for breast cancer diagnosis |
|
First visit |
65(32.5) |
Second visit |
96(48.0) |
Third visit |
30(15.0) |
Fourth visit and Fifth visit |
13(6.5) |
Total |
200(100) |
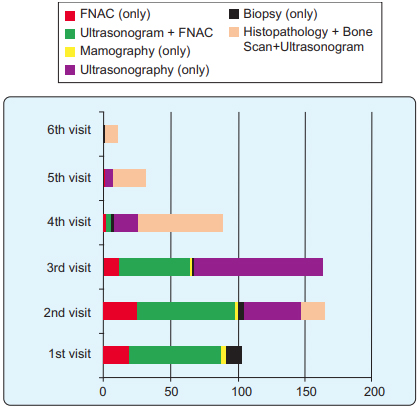
Of the total 200 patients, 71 (30.5%) patients time to diagnosis was for 1-6 months. Mean time to diagnosis was 11 months. Maximum diagnosis of breast cancer 140 (70%) was done at private hospital, 43 (21.5%) were diagnosed at public hospital (Medical College and District hospital) and only 17 (8.5%) at cancer hospital (table-I). Maximum respondents 95 (47.5%) 1st sought help from the homeopathy, 67(33.5%) respondents sought help to past graduate doctor, only 38 (19.0%) respondents consulted to MBBS physician In total, 65 (32.5%) patients diagnosed as breast cancer in 1st visit. Maximum 96 (48.0%) patients were diagnosed in 2nd visit. After clinical examination one to six visits was required for laboratory diagnosis to confirm breast cancer. FNAC was done individually or along with ultra sonogram. A total of 52 (26.0%), 49 (24.5%), 20 (10%) patients were done both ultrasonogram and FNAC at 1st, 2nd and 3rd visit respectively beside this 43 (21.5%), 48 (24.0%), 18 (9.0%) patients was done biopsy at 2nd, 3rd and 4th visit respectively. As diagnostic purpose very few patients 7 (3.5%) had done mammography at early three visits. Maximum patients ultimately confirmed by histopathology at 3rd, 4th and 5th visits along with bone scan (Figure 1). Association of time to diagnosis with present treatment of the respondents was analyzed using Pearson’s Chi-square (c2) method and summarized in table II. Results showed that time to diagnosis had significant association with the caner stage (p<0.0001), 1st contact with health care service provider (p<0 .0001) and 1st diagnostic institution (p=.059), number of consultations for diagnosis (p<0 .0001) (table II).
Variables |
Time to diagnosis |
Comment X2, df=1 |
|
|---|---|---|---|
Within 6 months n (%) |
More than 6 months n (%) |
||
Cancer stage |
|
|
|
Early stage |
27 (73.5%) |
11 (26.5%) |
28.00 |
Late stage |
42(26.5%) |
120(73.5%) |
p<0.0001 |
1stHealth care service provider for clinical diagnosis |
|
|
|
Physicians |
50 (73.9%) |
55 (42.7%) |
18.00 |
Other than physicians |
20 (26.1%) |
75 (57.3%) |
p<0 .0001 |
1st diagnostic center |
|
|
|
Private |
50(81.2%) |
90(68.7%) |
3.50 |
Public |
15 (18.8%) |
45 (31.3%) |
p=.059 |
Number of consultations for diagnosis |
|
|
|
1st visit |
34 (52.4%) |
31 (47.6%) |
13.00 |
Other than 1st visit |
35(26.3%) |
100 (73.7%) |
p< 0.0001 |
In order to prediction of the effects of independent variable on time to diagnosis, logistic regression was used. Thought all logistic regression analysis odds ratio greater than 1.00 (OR>1.00) indicated increased likelihood of diagnostic delay. Conversely, odds ratio less than 1.00 (OR<1.00) indicated decreased likelihood of diagnostic delay. (Figure 2).
The logistic regression was performed to see the diagnostic delay with presentation of patients during diagnosis (table III). Stage of cancer was 7 times more likely to cause diagnostic delay (OR=19.749; 95% CI 3.206-19.749) p<0.0001. First consultation with health care provider had 3 times more likely cause delay in breast cancer diagnosis. Diagnostic visits was less likely to cause delay (OR=0.426; 95% CI 0.188-0.965) p=0.041.
Factors influences the laboratory diagnosis |
OR |
95%CI for OR |
pvalue |
||
|---|---|---|---|---|---|
Stage of cancer |
Stage I & II |
Reference group |
|
|
|
Stage III & IV |
7.957 |
3.206 |
19.749 |
0.000 |
|
First health care provider |
Physician |
Reference group |
|
|
|
Other than Physician |
3.862 |
1.877 |
7.944 |
0.000 |
|
Diagnostic institution |
Private |
Reference group |
|
|
|
Public hospital |
0.552 |
0.243 |
1.250 |
0.154 |
|
Number of Fine-Needle |
One time |
Reference group |
|
|
|
Aspiration Cytology |
More than one time |
1.829 |
0.867 |
3.860 |
0.113 |
Number of diagnostic visit |
1st visit |
Reference group |
|
|
|
More than 1st visit |
0.426 |
0.188 |
0.965 |
0.041 |
|
Discussion
Diagnosing breast cancer usually begins when a lump is found in breast or a screening mammography suggests a problem with the breast, but in developing country ultrasonography is one of a choice.17 Shieh SH found that women who received an MRI examination on first visit also had the disease diagnosed much earlier compared with those without the test (8.4 vs. 28.9 days; p < 0.001).18 But in this study, a total of 154 (77.0%) patients did Fine-Needle Aspiration Cytology (FNAC) as a first choice for diagnosis. Ultra sonogram was the second choice one. Goodson WH found that Fine-Needle Aspiration is the least invasive way to obtain tissue, but due to untrained physician, one percent women undergo delay .19 In this study, it was showed that FNAC was not always accurate for that, one fourth of the patients repeated FNAC for 2-3 times. Delay was associated with a benign mammography report (relative risk, 10.8; 95% confidence interval, 5.1-22.8), a woman finding her own mass (relative risk, 3.3; 95% confidence interval, 1.8-6.2), and current hormone replacement therapy (relative risk, 3.1; 95% confidence interval, 1.2-8.5).19 In this study, diagnostic delay was associated with the cancer stage and type of 1st diagnostic centre (p=.059), number of consultation for diagnosis (p<0 .0001).
Shieh SH found that number of hospitals visits was also associated with the delay in diagnosis. It took 10 times longer to have the breast cancer diagnosed for women visiting three hospitals compared with women visiting only one hospital (147.4 vs. 14.3 days; p < 0.001).18 As because, patients had already in advanced stage, to reduce system loss and rapid diagnosis as well easy accessibility of health services, three fourth patients attended at private hospital.
Norsa’adah found that the median time to diagnosis was 5.5 months. The frequency of diagnosis delay of more than 3 months was 72.6% and delay of more than 6 months occurred in 45.5% of the cases. The factors associated with diagnosis delay included the use of alternative therapy (odds ratio (OR) 1.77; 95% confidence interval (CI): 1.06, 2.94), breast ulcer (OR 5.71; 95% CI: 1.59, 20.47), palpable axillary lymph nodes (OR 2.19; 95% CI: 1.23, 3.90), false-negative diagnostic test (OR 5.32; 95% CI: 2.32, 12.21), non-cancer interpretation (OR 1.68; 95% CI: 1.01, 2.78) and negative attitude towards treatment (OR 2.09; 95% CI: 1.15, 3.82).7 Ermiah E also found that the median of diagnosis time was 7.5 months. Only 30.0% of patients were diagnosed within 3 months after symptoms. 14% of patients were diagnosed within 3–6 months and 56% within a period longer than 6 months. A number of factors predicted diagnosis delay: symptoms were not considered serious in 27% of patients. Inappropriate reassurance that the lump was benign was an important reason for prolongation of the diagnosis time. Diagnosis delay was associated with initial breast symptom (s) that did not include a lump (p < 0.0001), with women who did not report monthly self examination (p < 0.0001), with old age (p = 0.004), with illiteracy (p = 0.009), with history of benign fibrocystic disease (p = 0.029) and with women who had used oral contraceptive pills longer than 5 years (p = 0.043). At the time of diagnosis, the clinical stage distribution was as follows: 9.0% stage I, 25.5% stage II, 54.0% stage III and 11.5% stage IV. Diagnosis delay was associated with bigger tumor size (p <0.0001), with positive lymph nodes (N2, N3; p < 0.0001), with high incidence of late clinical stages (p < 0.0001), and with metastatic disease (p < 0.0001).20 In this study, it was to be found that the mean of diagnostic delay was 11 months with influencing factors were, all the respondents 200 (100%) had lack of knowledge on breast cancer, 95%(n=190) had wrong perception, 122 (61.0%) respondents were delayed due to mentally upset, 157 (78.5%) had economic cause to delay in diagnosis, 123 (61.5%) had lack of social support , 148 (74.0%) had poor health care service delivery and utilization and 111 (55.5%) delayed due to received alternative treatment, however transportation factor was not the cause of delay. Abu-Helalah found that patients with diagnosis delay were 49.1%. The main reported reasons for delay in presentation were ignorance of the nature of the problem (65.6%), limited/lack of knowledge that symptoms were suggestive of cancer diagnosis (16.7%), and misdiagnosis (16.7%). 14 Toure also found that lack of financial means (36%), cultural habits with first intent traditional treatment (41.1%), misdiagnosis (7.1%) and lack of therapeutic care cause delay in diagnosis.21
Conclusion
Diagnosis of breast cancer usually starts with a lump on breast or axilla. Patient herself or family member wasted time to take decision to whom and where they go first for seeking medical help. After appearing the symptom of breast cancer patients should know where she go and what to do. There should be a proper guideline of investigation for accurate diagnosis of breast cancer. Avoid repeated investigation trained and skilled personnel should be required.
Acknowledgments
Authors acknowledge to Professor Md. Ziaul Islam, Department of Community Medicine, NIPSOM and Professor Md. Mizanur Rahman for their valuable suggestions to conduct this study.
References
- Stewart B, Kleihues PE. World Cancer Report. Lyon, France: IARC Press. 2003
- International Agency for Research on Cancer Working Group on the Evaluation of Cancer-Preventive Strategies. Handbooks of Cancer Prevention, vol. 7, Breast Cancer Screening. Lyon, France: IARC Press. 2002
- FerlayJ, Bray, F, Pisani, P, Parkin, DM. GLOBOCAN 2002. Cancer Incidence, Mortality and Prevalence Worldwide. Version 2.0. Lyon: IARC Pres. 2004
- Rahman, M, Ahsan A, Begum F, Rahman K. Epidemiology, risk factors and Tumor profiles of breast Cancer in Bangladeshi underprivileged women. The Gulf Journal of Oncology. 2015; 17:34-42.
- Story HL, Love RR, Salim R, Roberto AJ, Krieger JL, Ginsburg OM. Improving Outcomes from Breast Cancer in a Low-Income Country: Lessons from Bangladesh. International Journal of Breast Cancer,2012, Article ID 423562, 9pages.
DOI:10.1155/2012/423562 - Hussain SA, Sullivan R. Review Article: Cancer Trends in Asia Cancer Control in Bangladesh. Jpn J Clin Oncol. 2013; 43:1159–1169.
DOI:10.1093/jjco/hyt140 - Norsa’adah B, Rampal KG , Rahmah MA , Naing NN, Biswal BM. Diagnosis delay of breast cancer and its associated factors in Malaysian women. BMC Cancer. 2011; 11:141.
Available from: www.biomedcentral.com/1471-2407/11/141 - Akhtar K, Akhtar K, Rahman M, Use of alternative Medicine is Delaying Health –Seeking Behavior By Bangladeshi Breast Cancer Patients. Eur J Breast Health 2018;14:166-172
DOI:10.5152/ejbh.2018.3929 - Burgess C, Hunter MS, Ramirez AJ. A qualitative study of delay among women reporting symptoms of breast cancer, Br J Gen Pract, 2001; 51:967-71.
- Bourdeanu L, Luu T, Baker N, Swain-Cabriales S, Chung CT, Mortimer J, Hurria A, Helton S, Smith D, Ferrell B, Juarez G, Somlo G. Barriers to Treatment in Patients With Locally Advanced Breast Cancer J Natl Compr Canc Netw. 2013; 11: 1193–98.
- Adah BN, Rahmah MA, Rampal KG, Knight A. Understanding Barriers to Malaysian Women with Breast Cancer Seeking Help. Asian Pacific J Cancer Prev. 2012; 13: 3723-30.
- Karbani G, Lim JNW , Hewison J, Atkin K, Horgan K, Lansdown M, Chu CE . Culture, Attitude and Knowledge about Breast Cancer and Preventive Measures: a Qualitative Study of South Asian Breast Cancer Patients in the UK. Asian Pacific J Cancer Prev. 2011; 12: 1619-26.
- MháthunaMN.‘Women’s Help Seeking Behaviour and The Associated Influencing Factors on Self Discovery of a Breast Symptom (internet). University Cork.,College 2011 Available at UCC Library: http://library.ucc.ie/ record=b2031138-S0.
- Abu-HelalahAM, Alshraideh AH, Al-Hanaqtah M, Da’na M, Al-Omari A, Mubaidin R, Delay in Presentation, Diagnosis, and Treatment for Breast Cancer Patients in Jordan, The Breast Journal, 2016;22:213–217
DOI:10.1111/tbj.12541 - Hamilton JB, Moore CE, Powe BD, Agarwal M, Martin P. Perceptions of Support Among Older African American Cancer Survivors. Oncol Nurs Forum. 2010; 37: 484–93.
DOI:10.1188/10.ONF.484-493 - Bish A, Ramirez A, Burgess C, Hunter M. Understanding why women delay in seeking help for breast cancer symptoms. Journal of Psychosomatic Research. 2005; 58: 321-26.
- http://www.cancer.ca/en/cancer-information/cancer-type/ breast/diagnosis/?region=on Diagnosis of breast cancer Canadian cancer society, 13/2/18.
DOI:www.cancer.ca/en/cancer-information/cancer-type/ breast/diagnosis/ - Shieh SH , Hsieh VC R, Liu SH, Chien C R, Lin C C, Wu T N. Delayed time from first medical visit to diagnosis for breast cancer patients in Taiwan. Journal of the Formosan Medical Association, 2014; 113: 696-703.
- Goodson WH, Moore DH. Causes of Physician Delay in the Diagnosis of Breast Cancer. Arch Intern Med. 2002; 162:1343-1348
DOI:10.1001/archinte.162.12.1343 - Ermiah E, Abdalla F, Buhmeida A, Larbesh E, Seppo P, Collan Y. Diagnosis delay in Libyan female breast cancer. BMC Research Notes. 2012; 5: 452.
Available from:www.Biomedcentral.com/1756-0500/5/452 - Toure M , Nguessan E, Bambara AT, Kouassi YKK, Dia JML, Adoubi I. Factors linked to late diagnosis in breast cancer in Sub-Saharan Africa: Case of Coˆted’Ivoire,Gyne´ cologieObste´ trique & Fertilite´. 2013; 41 : 696–700.
National Institute of Preventive and Social Medicine (NIPSOM), Dhaka, Bangladesh.
khurshedaakhter11588@gmail.com
 0000-0003-2456-9472
0000-0003-2456-9472
Submission
21 September 2020
Accepted
30 June 2021
Published
1 August 2021
Apply citation style format of Bangladesh Medical Research Council
Issue
Vol 47 No 2 (2021)
Section
Research Articles
Ethical Clearance
IRB of NIPSOM, Dhaka, Bangladesh.
Financial Support
None
Conflict of Interest
No conflict of interest.