Principal Contact
Abstract:
Urolithiasis is the third most common disease of the urinary tract. Among all urinary tract stones, majorities are ureteral stones located in the distal part of the ureters. At present, multimodalities of treatment are available to the urologists. The purpose of the present study was to observe the efficacy of Tamsulosin in conventional treatment of juxtavesical ureteric stone having size up to 8 mm. This was a single centered, parallel randomized control trial carried out in the outpatient department of Urology, Bangabandhu Sheikh Mujib Medical University (BSMMU), Dhaka from July 2007 to June 2008. The patients with unilateral, juxtavesical ureteral stone with normal functioning kidney and absence of clinical and laboratory signs of urinary tract infection and stone size up to 8 mm were included in the study. Patients were divided into two groups according to the computer generated simple random sampling. Patients of Group-A were given conventional hydrotherapy treatment and patients of Group-B were given Tamsulosin 0.4mg/day along with the conventional hydrotherapy. Each patient was followed-up weekly until stone expulsion for 4 weeks. In Group-A and Group-B, the mean age with SD was 38.55±10.05 and 37.7±9.33 years. Expulsion occurred in 32 (53.33%) of 60 patients in Group-A and 51 (85%) of 60 patients in Group-B (p <0.05). The number of pain episodes in this study was statistically significantly lower in Group-B patients compared to Group-A (p<0.05). Urinary tract infection was encountered in 12 (20%) patients of Group-A and 2 (3.33%) patients of Group-B (p<0.05) during four weeks therapy which was treated by appropriate antibiotics. No side effects of Tamsulosin were encountered in any patients of Group-B which could require the cessation of the medication or might need for dose titration. Findings of the study revealed that the Tamsulosin supplemented conventional therapy is more effective than conventional hydrotherapy alone in management of juxtavesical ureteral stones.
Key words:Juxtavesical ureteral stones; Tamsulosin; Medical management; Randomized control trial.
Key words:Juxtavesical ureteral stones; Tamsulosin; Medical management; Randomized control trial.
Introduction:
Stone disease is one of the most common afflictions of modern society. Urolithiasis affects 4-15% of world population and the incidence of this disease is increasing day by day.2 Of all the urinary tract stones, 20% are ureteral stones, and 70% of these ureteral stones are found in the distal part of the ureters.3 The goal of treatment of patients suffering from ureteral calculi is to achieve complete stone clearance with minimal morbidity. At present, multimodalities of treatment are available to the urologists like expectant treatment, noninvasive procedure like extracorporeal shockwave lithotripsy, minimal invasive procedures like ureteroscopy or laparoscopy and open surgical intervention.4
Ureteral calculi of any size may be associated with renal obstruction and care must be taken to prevent irreversible damage to kidney, whether patient selects expectant or active treatment.4 An expectant treatment or watchful waiting approach may be expected to produce spontaneous stone expulsion up to 50% of cases but some complications such as urinary infection, hydronephrosis, and repetitive colicky pain may occur.5,6 Noninvasive treatment with extracorpo-real shockwave lithotripsy and minimal invasive approach with ureteroscopy allow ureterolithiasis to resolve in almost all cases but these procedures are not risk free and they require some experience and not cost effective.5,7 On the contrary, the role of medical expulsive ther-apy in the treatment of this pathological condition is still unclear.8 In particular, the most effective treatment regimen for spontaneous stone expulsion and control of painful symptoms have not been yet determined despite the widespread need in clinical practice. Although each alternative has some advantages and disadvantages, none guarantees a stone-free state, which depends on many factors.9 Although stone size and location are the main factors affecting stone clearance, the internal anatomic structure of the ureter and stone composition also seem to be unmodifiable factors. In the distal ureter, seventy one to ninety eight percent of stones of < 5mm and 25-53% stones with a diameter of 5-10 mm are reported to pass spontaneously with watchful waiting approach.5
Tamsulosin, an alpha1- adrenergic antagonist usually used in symptomatic case of BPH owing to its inhibitory effect on alpha1A receptors in relaxing prostatic and bladder neck smooth muscles.10 It has also effect on alpha1D adrenoceptors of ureteric smooth muscles in facilitating expulsion of stone from its juxtavesical part.11 Few studies in different countries have been performed to evaluate the role of Tamsulosin in facilitating expulsion of juxtavesical ureteral stones. But so far no such study has been undertaken in this country. For this reason, this prospective study was performed to assess the role of alpha1 adrenoceptos antagonist Tamsulosin in facilitating the spontaneous expulsion of juxtavesical ureteral stones.
Stone disease is one of the most common afflictions of modern society. Urolithiasis affects 4-15% of world population and the incidence of this disease is increasing day by day.2 Of all the urinary tract stones, 20% are ureteral stones, and 70% of these ureteral stones are found in the distal part of the ureters.3 The goal of treatment of patients suffering from ureteral calculi is to achieve complete stone clearance with minimal morbidity. At present, multimodalities of treatment are available to the urologists like expectant treatment, noninvasive procedure like extracorporeal shockwave lithotripsy, minimal invasive procedures like ureteroscopy or laparoscopy and open surgical intervention.4
Ureteral calculi of any size may be associated with renal obstruction and care must be taken to prevent irreversible damage to kidney, whether patient selects expectant or active treatment.4 An expectant treatment or watchful waiting approach may be expected to produce spontaneous stone expulsion up to 50% of cases but some complications such as urinary infection, hydronephrosis, and repetitive colicky pain may occur.5,6 Noninvasive treatment with extracorpo-real shockwave lithotripsy and minimal invasive approach with ureteroscopy allow ureterolithiasis to resolve in almost all cases but these procedures are not risk free and they require some experience and not cost effective.5,7 On the contrary, the role of medical expulsive ther-apy in the treatment of this pathological condition is still unclear.8 In particular, the most effective treatment regimen for spontaneous stone expulsion and control of painful symptoms have not been yet determined despite the widespread need in clinical practice. Although each alternative has some advantages and disadvantages, none guarantees a stone-free state, which depends on many factors.9 Although stone size and location are the main factors affecting stone clearance, the internal anatomic structure of the ureter and stone composition also seem to be unmodifiable factors. In the distal ureter, seventy one to ninety eight percent of stones of < 5mm and 25-53% stones with a diameter of 5-10 mm are reported to pass spontaneously with watchful waiting approach.5
Tamsulosin, an alpha1- adrenergic antagonist usually used in symptomatic case of BPH owing to its inhibitory effect on alpha1A receptors in relaxing prostatic and bladder neck smooth muscles.10 It has also effect on alpha1D adrenoceptors of ureteric smooth muscles in facilitating expulsion of stone from its juxtavesical part.11 Few studies in different countries have been performed to evaluate the role of Tamsulosin in facilitating expulsion of juxtavesical ureteral stones. But so far no such study has been undertaken in this country. For this reason, this prospective study was performed to assess the role of alpha1 adrenoceptos antagonist Tamsulosin in facilitating the spontaneous expulsion of juxtavesical ureteral stones.
Materials and Methods:
Study design and Population: This was a single centred, parallel, double blind randomized control trial. This study was carried out in the Outpatient Department of Urology, BSMMU, Dhaka from July 2007 to June 2008. The patients with both sexes above 18 years of age with unilateral, juxtavesical ureteral stone with normal functioning kidney and absence of clinical and laboratory signs of urinary tract infection and stone size up to 8 mm were included in this study. Before recruitment, for baseline data, each patient was evaluated by history, physical examination and investigations like urine routine and microscopic examination, culture and sensitivity test, serum creatinine measurement, intravenous urography, ultrasonography of KUB and prostate and other biochemical and haematological tests. A data sheet was used to record the information. Patients with multiple stones, severe hydronephrosis with a history of spontaneous stone expulsion, distal ureteral surgery, diabetes mellitus, peptic ulcer disease, hypotension, patients getting calcium antagonists, stone size more than 8 mm, and anatomical deformity at vesicoureteric junction, single kidney and bladder outflow obstruction were excluded from this study.
Randomization: All the patients fulfilling the inclusion and exclusion criteria were recruited. After duly taking written informed consent patients were divided into two groups which were generated randomly by software and were named as Group-A and Group-B.
Intervention: Patients of Group A were given conventional treatment consisted of hydration with minimum two liter water intake daily, physical exertion and analgesics if required (50mg diclofenac sodium suppository with H2 blocker). On the other hand, patients of Group-B were given Tamsulosin 0.4mg/day along with the conventional treatment. Each of the patients continued the therapy.
Follow up and outcome measures: Each patient was followed-up weekly until stone expulsion for four weeks. All patients of both groups were asked during weekly follow-up about stone expulsion time, episodes of colic, analgesic use and side effects of drug. Follow up cases were seen in urology outpatient department. In each of the follow-up study history, clinical examination, urine routine microscopic examination, plain X-ray of KUB region and ultrasonography of KUB region were done and data on stone expulsion were recorded in data sheet. The criteria for treatment discontinuation as well as the need of hospitalization and/or endoscopic treatments were pain uncontrolled by analgesic therapy, fever, progressive hydronephrosis, increased creatinine level, unsuccessful expulsion after four weeks and patient desired to remove the stone before day 28.
Ethical consideration: Prior to the commenc-ement of the study, the research protocol was approved by the Ethical Committee of BSMMU
Statistical Analysis: Collected data were edited by meticulous checking and rechecking. Statistical Package for Social Science (SPSS), a statistical analysis package program version-17 was used. Measures of dispersion (mean, standard deviation) and the tests of significance (paired t test, student's unpaired t test, Z test and X2 test) were employed to examine the statistical significance of the study. A p value <0.05 was taken as minimum level of significance.
Study design and Population: This was a single centred, parallel, double blind randomized control trial. This study was carried out in the Outpatient Department of Urology, BSMMU, Dhaka from July 2007 to June 2008. The patients with both sexes above 18 years of age with unilateral, juxtavesical ureteral stone with normal functioning kidney and absence of clinical and laboratory signs of urinary tract infection and stone size up to 8 mm were included in this study. Before recruitment, for baseline data, each patient was evaluated by history, physical examination and investigations like urine routine and microscopic examination, culture and sensitivity test, serum creatinine measurement, intravenous urography, ultrasonography of KUB and prostate and other biochemical and haematological tests. A data sheet was used to record the information. Patients with multiple stones, severe hydronephrosis with a history of spontaneous stone expulsion, distal ureteral surgery, diabetes mellitus, peptic ulcer disease, hypotension, patients getting calcium antagonists, stone size more than 8 mm, and anatomical deformity at vesicoureteric junction, single kidney and bladder outflow obstruction were excluded from this study.
Randomization: All the patients fulfilling the inclusion and exclusion criteria were recruited. After duly taking written informed consent patients were divided into two groups which were generated randomly by software and were named as Group-A and Group-B.
Intervention: Patients of Group A were given conventional treatment consisted of hydration with minimum two liter water intake daily, physical exertion and analgesics if required (50mg diclofenac sodium suppository with H2 blocker). On the other hand, patients of Group-B were given Tamsulosin 0.4mg/day along with the conventional treatment. Each of the patients continued the therapy.
Follow up and outcome measures: Each patient was followed-up weekly until stone expulsion for four weeks. All patients of both groups were asked during weekly follow-up about stone expulsion time, episodes of colic, analgesic use and side effects of drug. Follow up cases were seen in urology outpatient department. In each of the follow-up study history, clinical examination, urine routine microscopic examination, plain X-ray of KUB region and ultrasonography of KUB region were done and data on stone expulsion were recorded in data sheet. The criteria for treatment discontinuation as well as the need of hospitalization and/or endoscopic treatments were pain uncontrolled by analgesic therapy, fever, progressive hydronephrosis, increased creatinine level, unsuccessful expulsion after four weeks and patient desired to remove the stone before day 28.
Ethical consideration: Prior to the commenc-ement of the study, the research protocol was approved by the Ethical Committee of BSMMU
Statistical Analysis: Collected data were edited by meticulous checking and rechecking. Statistical Package for Social Science (SPSS), a statistical analysis package program version-17 was used. Measures of dispersion (mean, standard deviation) and the tests of significance (paired t test, student's unpaired t test, Z test and X2 test) were employed to examine the statistical significance of the study. A p value <0.05 was taken as minimum level of significance.
Result:
A total of 246 patients were assessed for eligibility of which 135 patients were selected as study population. Among them 7 patients were withdrawn before randomization due to non-cooperation. The remaining 128 patients were randomly allocated into Group A consisted of 64 patient and Group B of 64 patients. During the study period 4 patients from Group-A and 4 patients from Group-B discontinued the intervention. Hence, they were dropped out and finally results of 60 cases from each group were compared. The mean age (±SD) for group A was 38.5 (SD±10.05) years (age range 18-60 years) and for Group B was 37.7 (SD±9.33) years (age range 18-59 years). Age of the patients of each group were compared and found no significant difference (table I).
In Group-A, 19 (31.7%) patients were in stone size between 3 to 5 mm and 41(68.3%) patients were in stone size between 6 to 8mm. In Group-B, 18 (30%) patients were in stone size between 3 to 5 mm and 42 (70%) patients were in stone size between 6 to 8 mm. In both groups, the distribution of stone size showed no statistical significance (table II).
In group A and B rate of stone expulsion from the ureter were 53.3% cases and 85.0% cases respectively. There was significant difference in clearance of stone between the groups (table III), but the rate of expulsion varies according to size shown in Figure 1 and Figure 2.
Figure 1: Rate of expulsion in smaller stone (3-5 mm)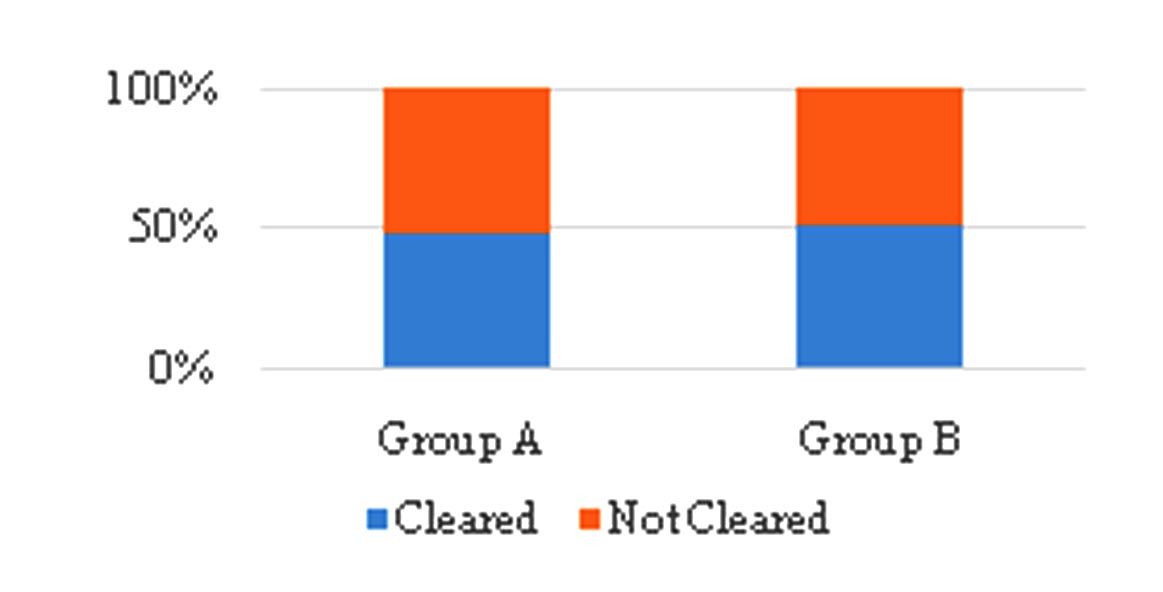
Figure 2: Rate of expulsion in larger stones (6-8 mm)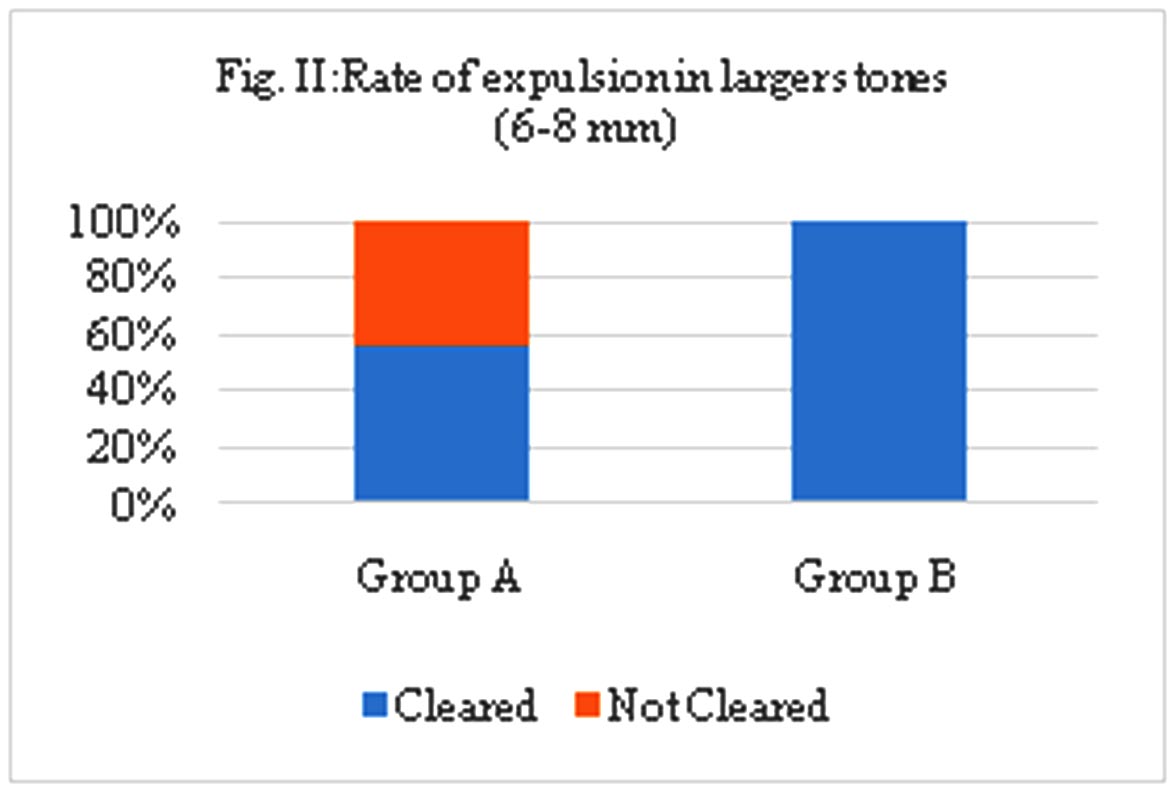
The mean episodes of pain in patients of Group A and Group B were respectively 4.13±1.704 and 2.58±1.519, shown in table IV;
Difference was statistically significant (p ±0.05). In group A and B urinary tract infection was detected in 20% and 3.33% patients respectively and the difference was statistically significant (p±0.05).
However, this treatment may not always be sufficient, especially for stones located at the intramural ureter, where smooth muscle tonus is more evident.13 Studies have revealed that alpha1-adrenergic receptors are the most abundant receptors in ureteral smooth muscle cells and alpha1-adrenergic antagonists inhibit basal tone, peristaltic activity and ureteral contractions.8 Generally, the main obstacle to the transport of lower ureteral stones is the intramural detrusor tunnel;7 thus, blocking these receptors could affect stone passage. Tamsulosin is a competitivealpha1-adrenergic antagonist having higher affinity for alpha1A and alpha1D adrenoceptors.These receptors are located in smooth muscle of prostate, bladder neck, detrusor, vesicoureteric junction and ureter specially lower part.12 The blockade of alpha adrenergic receptor by a specific antagonist like Tamsulosin results in decreased ureteralperistaltic amplitude and frequency with a consequent loss of intraureteral pressure and thereby an increase in fluid transport ability. Thus the effect of Tamsulosin on the obstructed ureter is to induce an increase in the intramural perssure gradient around the stone as well as decreased peristalsis below the ureter and consequently a dcrease in intramural pressure below the stone in association with the decrease in basal and micturition pressure even at the bladder neck. All these mechanisms bolster the urge to expel the stone.11,16
The present study was designed to prove the efficacy of Tamsulosinin addition to conventional treatment for the management of juxtavesical ureteric stone having size up to 8 mm. A total of 120 patients were grouped into two on alternate basis, 60 patients in group A treated with conventional therapy consists of hydration, physical exertion and analgesics. 60 patients of group B were given Tamsulosin 0.4mg daily along with the conventional treatment. Therapies in both groups continued for 4 weeks or until stone expulsion within 4 weeks. In complete obstruction, the signs of renal injury appear in three to four weeks. For this reason, the spontaneous passage of stones can be waited on for 4 weeks.3 The mean age with SD in Group-A and Group-B were 38.55±10.05 and 37.7±9.33 years. No significant difference was observed among the two groups in relation to age and sex. This creates an equal group, so that these didn't cause any effect to the outcomes.
In this study, mean stone size was 5.88±1.23 mm (range 3-8) for Group-A and 5.94±0.92 mm (range 3.5-8) for Group-B. There was no significant difference between two groups with respect to stone size. The above distribution correlates with the study done by Cervenakov et al14 having stone size between 3-10 mm in each group but does not correlate with the study conducted by Dellabella et al11 having stone size 4-11mm and 3.8-13 mm in conventional and Tamsulosin group respectively.
Episodes of pain in this study was statistically significantly lower in Group-B patients compared to Group-A (p <0.05). Mean episodes of pain in patients of Group-A was 4.13± 1.704 and that in Group-B was 2.58± 1.519.Patients in the study by Yilmaz E et al12 suffered from pain episodes of 2.42±1.39 and 1.72±0.88 without and with Tamsulosin respectively.
In the current study, stone expulsion occurred in 83(69.2%) of 120 subjects enrolled. Expulsion occurred in 32 (53.3%) of 60 patients in Group-A and 51 (85.0%) of 60 patients in Group-B. Statistical analysis showed a significantly higher stone expulsion rate in Group-B compared with Group-A (p <0.05) which is more or less similar to the study conducted by Cervenakov et al14 where stone expulsion rate was 62.8% in standard treatment group and 80.4% in group where standard treatment was supplemented by Tamsulosin. Similarly, study conducted by Yilmaz E et al12 Tamsulosin group showed 79.31% stone expulsion in comparison to 53.57% stone expulsion in group without Tamsulosin. A meta-analysis done by Lu Zet al17 worked on twenty-nine trials with a total of 2,763 patients. The pooled analysis showed a19% improvement in stone clearance with tamsulosin. But Dellabella M et al11 in a study showed stone expulsion rates were 100% and 70% in group treated with and without Tamsulosin respectively, These high rates of stone expulsion might be due to use of steroid (Deflazacort) in both groups.
In this study, effect of stone size on expulsion rate was observed. In smaller stones (3-5mm range), Group-A and Group-B included 19 and 18 patients respectively. Expulsion occurred in 9 (47.36%) patients of Group-A and 9 (50%) patients of Group-B; difference was not statistically significant (p >0.05) but in relation to larger stones (6-8mm range), expulsion seen in 23 (56.09%) patients of Group-A and 42 (100%) patients of Group-B, difference was significant (p < 0.05). A systematic review by Somani BK et al15 claimed a result similar to our finding. But Dellabella M et al11 in their study did not find any correlation between stone size and expulsion rate of stone.
In this study, complications like urinary tract infection, repeated colicky pain were encountered during study period. Urinary tract infection was encountered in 12(20%) patients of Group-A and 2(3.33%) patients of Group-B during four weeks therapy and was treated by appropriate antibiotics. Difference is statistically significant (p <0.05). Above findings correlate with different studies conducted by Cervenakov et al,14 Dellabella et al11 and Yilmaz E et al.12 No serious side effects of Tamsulosin were encountered in any patients of either group, which could require the cessation of the medication or need for dose titration. Ten patients of Group-A and 8 patients of Group-B complained of mild headache and palpitation. In studies conducted by Dellabella et al and Porpiglia et al to enable spontaneous passage of distal ureteral stones, steroids have generally been included in medical treatment. However, in this study no steroid was used. The steroid sparing approach was another important feature of this study.
Conclusion:
Tamsulosin has a potentially important role for conservative expulsive therapy of juxtavesical ureteral stones, broadening pharmacological indications rather than endoscopic treatments for the resolution of this disease. Considering the findings of the present study and the studies previously done by others, it may be concluded that Tamsulosin supplemented conventional therapy is more effective than conventional hydrotherapy alone in the management of juxtavesical ureteral stones. Further studies are recommended to validate the promising and statistically significant results of this study.
A total of 246 patients were assessed for eligibility of which 135 patients were selected as study population. Among them 7 patients were withdrawn before randomization due to non-cooperation. The remaining 128 patients were randomly allocated into Group A consisted of 64 patient and Group B of 64 patients. During the study period 4 patients from Group-A and 4 patients from Group-B discontinued the intervention. Hence, they were dropped out and finally results of 60 cases from each group were compared. The mean age (±SD) for group A was 38.5 (SD±10.05) years (age range 18-60 years) and for Group B was 37.7 (SD±9.33) years (age range 18-59 years). Age of the patients of each group were compared and found no significant difference (table I).
Table I: Mean Age of the patients in study groups
Group |
Mean±SD |
p value* |
Group A |
38.5±10.05 |
>0.05 |
Group B |
37.7±9.33 |
In Group-A, 19 (31.7%) patients were in stone size between 3 to 5 mm and 41(68.3%) patients were in stone size between 6 to 8mm. In Group-B, 18 (30%) patients were in stone size between 3 to 5 mm and 42 (70%) patients were in stone size between 6 to 8 mm. In both groups, the distribution of stone size showed no statistical significance (table II).
Table II: Distribution of mean stone size among the study population
Group |
Stone size Mean±SD (mm) |
Calculated |
pvalue |
Group A |
5.88±1.23 |
0.304ns |
>0.05 |
Group B |
5.94±0.92 |
In group A and B rate of stone expulsion from the ureter were 53.3% cases and 85.0% cases respectively. There was significant difference in clearance of stone between the groups (table III), but the rate of expulsion varies according to size shown in Figure 1 and Figure 2.
Table III: Rate of Stone expulsion in study groups
Group |
Stone expulsion |
Total |
Calculated |
p |
|
Group A |
32 |
28 |
60 |
|
|
Group B |
51(85%) |
9(15%) |
60 |
12.658* |
<0.05 |
Total |
83(70.8%) |
37(39.2%) |
120 |
|
|
Figure 1: Rate of expulsion in smaller stone (3-5 mm)
Figure 2: Rate of expulsion in larger stones (6-8 mm)
The mean episodes of pain in patients of Group A and Group B were respectively 4.13±1.704 and 2.58±1.519, shown in table IV;
Table IV: Pain episodes in two study groups
Group |
No. of sufferer |
Mean±SD |
Calculated Z value |
p value |
A |
48(80%) |
4.13±1.704 |
5.11s |
<0.05 |
B |
36(60%) |
2.58±1.519 |
Difference was statistically significant (p ±0.05). In group A and B urinary tract infection was detected in 20% and 3.33% patients respectively and the difference was statistically significant (p±0.05).
Discussion
Though there is no exact data about the prevalence of ureterolithiasis in Bangladesh but the problem is quite common. Multimodalities of treatment are available to the urologists. Minimal invasive therapies such as extracorporeal shockwave lithotripsy and ureteroscopy have been widely introduced for treatment of ureteric stones during last two decades.12 The efficacy of these treatments has been proved by several studies.13 However, although such procedures are rather effective, they are not free of risk or inconveniences and are quite expensive.5On the other hand, conventional treatment like simple watchful waiting approach with two litres of daily water intake can result in complications such as urinary tract infection, repeated colicky pain or hydronephrosis and can affect renal function.12However, this treatment may not always be sufficient, especially for stones located at the intramural ureter, where smooth muscle tonus is more evident.13 Studies have revealed that alpha1-adrenergic receptors are the most abundant receptors in ureteral smooth muscle cells and alpha1-adrenergic antagonists inhibit basal tone, peristaltic activity and ureteral contractions.8 Generally, the main obstacle to the transport of lower ureteral stones is the intramural detrusor tunnel;7 thus, blocking these receptors could affect stone passage. Tamsulosin is a competitivealpha1-adrenergic antagonist having higher affinity for alpha1A and alpha1D adrenoceptors.These receptors are located in smooth muscle of prostate, bladder neck, detrusor, vesicoureteric junction and ureter specially lower part.12 The blockade of alpha adrenergic receptor by a specific antagonist like Tamsulosin results in decreased ureteralperistaltic amplitude and frequency with a consequent loss of intraureteral pressure and thereby an increase in fluid transport ability. Thus the effect of Tamsulosin on the obstructed ureter is to induce an increase in the intramural perssure gradient around the stone as well as decreased peristalsis below the ureter and consequently a dcrease in intramural pressure below the stone in association with the decrease in basal and micturition pressure even at the bladder neck. All these mechanisms bolster the urge to expel the stone.11,16
The present study was designed to prove the efficacy of Tamsulosinin addition to conventional treatment for the management of juxtavesical ureteric stone having size up to 8 mm. A total of 120 patients were grouped into two on alternate basis, 60 patients in group A treated with conventional therapy consists of hydration, physical exertion and analgesics. 60 patients of group B were given Tamsulosin 0.4mg daily along with the conventional treatment. Therapies in both groups continued for 4 weeks or until stone expulsion within 4 weeks. In complete obstruction, the signs of renal injury appear in three to four weeks. For this reason, the spontaneous passage of stones can be waited on for 4 weeks.3 The mean age with SD in Group-A and Group-B were 38.55±10.05 and 37.7±9.33 years. No significant difference was observed among the two groups in relation to age and sex. This creates an equal group, so that these didn't cause any effect to the outcomes.
In this study, mean stone size was 5.88±1.23 mm (range 3-8) for Group-A and 5.94±0.92 mm (range 3.5-8) for Group-B. There was no significant difference between two groups with respect to stone size. The above distribution correlates with the study done by Cervenakov et al14 having stone size between 3-10 mm in each group but does not correlate with the study conducted by Dellabella et al11 having stone size 4-11mm and 3.8-13 mm in conventional and Tamsulosin group respectively.
Episodes of pain in this study was statistically significantly lower in Group-B patients compared to Group-A (p <0.05). Mean episodes of pain in patients of Group-A was 4.13± 1.704 and that in Group-B was 2.58± 1.519.Patients in the study by Yilmaz E et al12 suffered from pain episodes of 2.42±1.39 and 1.72±0.88 without and with Tamsulosin respectively.
In the current study, stone expulsion occurred in 83(69.2%) of 120 subjects enrolled. Expulsion occurred in 32 (53.3%) of 60 patients in Group-A and 51 (85.0%) of 60 patients in Group-B. Statistical analysis showed a significantly higher stone expulsion rate in Group-B compared with Group-A (p <0.05) which is more or less similar to the study conducted by Cervenakov et al14 where stone expulsion rate was 62.8% in standard treatment group and 80.4% in group where standard treatment was supplemented by Tamsulosin. Similarly, study conducted by Yilmaz E et al12 Tamsulosin group showed 79.31% stone expulsion in comparison to 53.57% stone expulsion in group without Tamsulosin. A meta-analysis done by Lu Zet al17 worked on twenty-nine trials with a total of 2,763 patients. The pooled analysis showed a19% improvement in stone clearance with tamsulosin. But Dellabella M et al11 in a study showed stone expulsion rates were 100% and 70% in group treated with and without Tamsulosin respectively, These high rates of stone expulsion might be due to use of steroid (Deflazacort) in both groups.
In this study, effect of stone size on expulsion rate was observed. In smaller stones (3-5mm range), Group-A and Group-B included 19 and 18 patients respectively. Expulsion occurred in 9 (47.36%) patients of Group-A and 9 (50%) patients of Group-B; difference was not statistically significant (p >0.05) but in relation to larger stones (6-8mm range), expulsion seen in 23 (56.09%) patients of Group-A and 42 (100%) patients of Group-B, difference was significant (p < 0.05). A systematic review by Somani BK et al15 claimed a result similar to our finding. But Dellabella M et al11 in their study did not find any correlation between stone size and expulsion rate of stone.
In this study, complications like urinary tract infection, repeated colicky pain were encountered during study period. Urinary tract infection was encountered in 12(20%) patients of Group-A and 2(3.33%) patients of Group-B during four weeks therapy and was treated by appropriate antibiotics. Difference is statistically significant (p <0.05). Above findings correlate with different studies conducted by Cervenakov et al,14 Dellabella et al11 and Yilmaz E et al.12 No serious side effects of Tamsulosin were encountered in any patients of either group, which could require the cessation of the medication or need for dose titration. Ten patients of Group-A and 8 patients of Group-B complained of mild headache and palpitation. In studies conducted by Dellabella et al and Porpiglia et al to enable spontaneous passage of distal ureteral stones, steroids have generally been included in medical treatment. However, in this study no steroid was used. The steroid sparing approach was another important feature of this study.
Conclusion:
Tamsulosin has a potentially important role for conservative expulsive therapy of juxtavesical ureteral stones, broadening pharmacological indications rather than endoscopic treatments for the resolution of this disease. Considering the findings of the present study and the studies previously done by others, it may be concluded that Tamsulosin supplemented conventional therapy is more effective than conventional hydrotherapy alone in the management of juxtavesical ureteral stones. Further studies are recommended to validate the promising and statistically significant results of this study.
References
- Margaret SP and Lotan Y. Urinary lithiasis: Etiology, Epidemiology and pathogenesis. In: Wein AJ, Kavoussi LR, Partin AW, Peters CA editors,: Campbell-Walsh Urology. 11th ed. Philadelphia: Elsevier; 2016. p 1170-74.
- Hesse A and Siener R. Current aspects of epidemiology and nutrition in urinary stone disease. World J Urol. 1997;15:165-71.
- Leavitt DA, Rosette JJ, Hoenig DM. Strategies for Nonmedical Management of Upper Urinary Tract Calculi. In Wein AJ, Kavoussi LR, Partin AW, Peters CA, editors: Campbell-Walsh Urology. 11thed. Philadelphia: Elsevier; 2016. p1250-54.
- Lingeman JE, Matlaga BR, Evan AP. Surgical management of upper urinary tract calculi. In. Kavoussi LR, Novick AC, Parton AW, Peters CA [editors]: Campbell-Walsh Urology. 9thed. Philadelphia: W.B. Saunders; 2007. p 1431-51
- Segura JW, Preminger GM, Assimos DG et al. Ureteral stones: Clinical Guidelines Panel summary report on the management of ureteral calculi. J Urol. 1997; 158: 1915-21.
- Miller OF, Kane CJ. Time to passage for observed ureteral calculi: A guide for patient education. J Urol. 1999; 162: 688-91.
- Lotan Y, Gettman MT, Roehrborn CG, Caddeu JA and Pearle,MS. Management of ureteral calculi: a cost comparison and decision making analysis. J Urol. 2002; 1620: 21.
- Dellabella M, Milanese G, Muzzonigro G. Randomized trial of the efficacy of Tamsulosin, Nifedipine and Phloroglucinol in medical expulsive therapy for distal ureteral stone. Journal of Urology. 2005; 174: 167-72.
- Whitfield HN. The management of ureteric stones. Part II: therapy. BJU International. 1999; 54(8): 916-21
- Yanardag H, Goktas S, Kibar Y Kilic S Erduran D. Intermittent Tamsulosin therapy in men with lower urinary tract symptoms. J Urol. 2005; 173: 155-58.
- Dellabella M, Milanese G, Muzzonigro G. Efficacy of Tamsulosin in the medical management of juxtavesical ureteral stones. Journal of Urology. 2003; 170: 2202-05.
- Yilmaz E, Batislam E, Basar MM, Tuglu D, Ferhat M, Basar H. The comparison and efficacy of 3 different adrenergic blockers for distal ureteral stones. J Urol. 2005; 173: 2010-2012.
- Kupeli B, Irkilatl L, Gurocak S, Tunc L, Kirac M, Karaoglan U et al. Does Tamsulosin enhance lower ureteral stone clearance with or without shockwave lithotripsy. Urology. 2004; 64: 1111-15.
- Cervenakov I, Fillo J, Mardiak J et al. Speedy elimination of ureterolithiasis in lower part of ureters with the alpha1-blocker tamsulosin. Int Urol Nephrol. 2002; 34: 25-29.
- Somani BK, Aboumarzouk O, Traxer O et al. Medical expulsive therapy for ureteral stones: where do we go from here? Nature Reviews Urology. 2016; 13:608-12.
- Campschroer T, Zhu Y, Duijvesz D, Grobbee DE, Lock MTWT. Alpha-blockers as medical expulsive therapy for ureteral stones. Cochrane Database of Systematic Reviews 2014; 4:
- Lu Z, Dong Z, Ding H, et al. Tamsulosin for Ureteral Stones: A Systematic Review and Meta-Analysis of a Randomized Controlled Trial. Urol Int. 2012; 89:107-15.